%201.svg)

Key Takeaways
- Multi-branch expansion multiplies billing complexity at rates exceeding revenue growth when RCM processes lack design specifications for distributed operation across locations, payer environments, and documentation systems.
- Denial rate variance of 2–3x between locations and AR aging concentrated in specific branches represent structural compliance failures, not staffing deficiencies. These indicators signal RCM processes that were never designed to meet scale requirements.
- Centralized governance must be implemented for medical coding, OASIS review, Medicare fee-for-service billing, and analytics. Functions requiring payer-specific expertise, including managed care billing, prior authorization, and patient communication, can be managed effectively by trained external teams, not just in-house local staff.
- The hybrid RCM model centralizes, where standardization ensures accuracy and retains local control, and contextual knowledge drives performance. This structure represents the configuration most multi-branch agencies require to stabilize reimbursement.
- Technology alignment represents a prerequisite for centralization, not a byproduct. Fragmented EHR platforms across branch locations must be resolved before structural RCM changes are implemented.
- Documentation standardization must precede coding centralization. The most common reason RCM centralization efforts fail involves centralizing coding before clinical documentation standards achieve uniformity across branches.
Expanding a home health agency from one location to multiple branches should ideally increase revenue opportunities. However, in reality, it often multiplies billing complexity at a faster rate than revenue growth.
Processes that work well in a single branch, such as shared documentation workflows, a small coding team, and billing staff familiar with payer contracts, begin to break down as the agency expands geographically. Each new branch introduces variations in payer mix and state Medicaid rules, leading to a fragmented revenue cycle with inconsistent operations that hinder benchmarking, auditing, and correction.
In multi-branch home health agencies, revenue cycle issues usually surface gradually as inconsistent denial patterns, delayed reimbursements tied to specific payer mixes, and reporting gaps that obscure the sources of revenue leakage.
For Revenue Cycle Management (RCM) directors and operations leads, the key challenge is deciding which RCM functions to centralize and which to keep local, while building scalable infrastructure that supports sustainable growth across multiple locations.
What this means operationally: Without a defined RCM structure, agencies lose visibility into where revenue risk originates.
The Scaling Dilemma: Why Adding Branches Breaks RCM
Most home health RCM breakdowns at scale are not caused by individual performance failures. They are caused by processes that were never designed to operate across multiple locations, payer environments, and documentation systems simultaneously.
When a single-branch agency grows, it typically carries its original workflows into new locations without redesigning them for distributed operation. Coding interpretation begins to vary between branches, authorization workflows diverge based on local payer requirements, and billing teams develop branch-specific workarounds that make reconciliation and performance comparison difficult at the organizational level.
The Patient-Driven Groupings Model (PDGM) compounds this. Under PDGM, reimbursement accuracy depends on precise clinical grouping, comorbidity coding, and timing thresholds. A coding error at one branch does not remain contained; it affects the agency's overall denial profile, audit exposure, and revenue forecasting accuracy.
Key Insight: RCM inconsistency across branches represents a structural problem, not a staffing problem. Resolving it requires a deliberate decision about which functions belong at the center and which belong in the field.
The Medicare Payment Advisory Commission (MedPAC) has recommended that CMS scrutinize home health agencies with unusual billing patterns, citing home health as a sector requiring additional safeguards due to its high-risk payment profile. Agencies operating across multiple locations face compounded audit risk when coding and documentation standards are not uniformly applied.
According to the HHS Office of Inspector General, CMS's Comprehensive Error Rate Testing (CERT) program recorded a 7.7% improper payment rate for home health claims in 2023, representing approximately $1.2 billion. While this figure reflects payment accuracy from the payer's perspective, the underlying causes, unsupported diagnosis codes and documentation deficiencies — are the same conditions that generate claim denials, trigger post-payment recoupments, and increase audit exposure for providers. Agencies that do not maintain consistent documentation standards across locations carry the highest share of that risk.
The OIG has launched a nationwide series of home health compliance audits, citing unsupported diagnosis codes and documentation deficiencies as the primary drivers. For multi-branch agencies, where documentation standards vary across locations, audit exposure is not evenly distributed; it concentrates in branches where coding governance is weak.
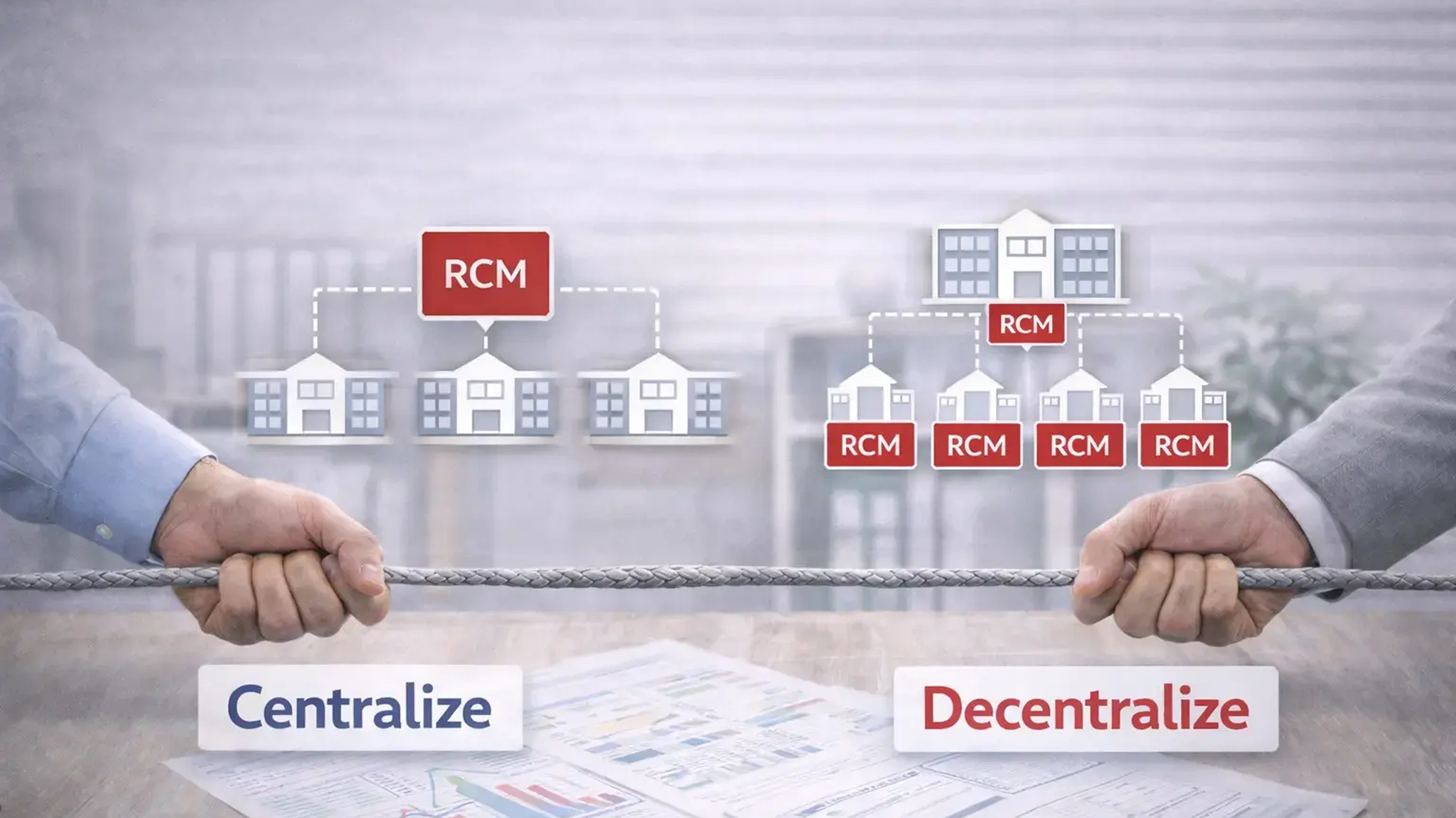
The Centralized RCM Model: Where It Works and Where It Does Not
Advantages of Centralization
A centralized RCM model consolidates coding, billing, compliance monitoring, and analytics under a single operational structure, either an internal shared services team or an outsourced partner, that serves all branch locations.
The operational advantages are significant. Standardization becomes enforceable rather than aspirational. Coding interpretation is governed by a single set of guidelines applied consistently across the organization. Compliance monitoring can be conducted against uniform benchmarks rather than location-by-location assessments. Analytics denial rates, days in accounts receivable (AR), claim turnaround time, pre-bill review outcomes become meaningful at the aggregate level because the underlying data is generated through consistent processes.
Centralization also concentrates expertise. Rather than maintaining coding competency across multiple branch teams with varying training levels and turnover rates, the agency can build or access a specialized team whose performance is measurable and whose knowledge base remains current with CMS guidance, OASIS manual updates, and payer policy changes.
What centralization solves: Consistency in coding, documentation review, and analytics across all locations.
This is particularly relevant under PDGM, where small variations in coding interpretation can materially impact reimbursement consistency across branches.
Limitations of Full Centralization
Centralization creates distance. For functions that require direct knowledge of local payer contracts, regional Medicaid rules, or managed care authorization requirements, a centralized team operating without that context will make avoidable errors.
Managed care billing and prior authorization present the most complexity in multi-state operations. Authorization requirements, billing formats, and dispute processes vary significantly across regional plans. A centralized team operating without current knowledge of those variations will generate avoidable denials, making payer-specific expertise, not physical proximity, the actual operational requirement.
Patient-facing communication, eligibility verification, coverage explanations, balance billing inquiries, similarly requires familiarity with local payer structures and care context. Whether that familiarity resides in on-site staff or an external team trained on the agency's payer mix and patient population is an operational decision, not a structural one.
The Decentralized RCM Model: Where It Works and Where It Breaks Down
Advantages of Decentralization
Decentralized RCM maintains billing and coding operations at the branch level, where staff have direct relationships with clinicians, immediate access to documentation, and working knowledge of local payer requirements.
For agencies operating in regions with complex managed care environments, where authorization requirements are frequent, contract terms vary significantly, and payer relationships require active management, billing staff with working knowledge of local plans provide operational agility that a generalist centralized team cannot easily replicate. That knowledge advantage is real; the question is whether it requires physical co-location or whether it can be built into a dedicated external team trained on the agency's specific payer environment.
Query resolution between coders and clinicians is faster when both operate within a shared workflow structure. When documentation clarifications require a formal query process, response timelines and accountability standards become operationally critical whether the coding team is down the hall or operating remotely with a defined escalation path.
Where Decentralization Creates Risk
Decentralized operations are structurally resistant to standardization. Each branch develops its own documentation practices, coding interpretations, and billing workflows. Over time, these diverge. Denial patterns at one location do not inform process corrections at another. Training is inconsistent. Staff turnover at a single branch can destabilize billing operations for months.
From a compliance standpoint, decentralization makes audit readiness significantly harder to maintain. When post-payment auditors review records across locations, they expect consistent documentation standards. When those standards vary, the agency cannot present a unified defense. Each branch becomes its own compliance exposure.
Benchmarking is also unreliable in a decentralized model. Denial rates, AR aging, and coding accuracy metrics measured at the branch level reflect local process variation as much as actual performance. Comparing results across locations, or against industry benchmarks, requires a level of data consistency that decentralized operations rarely produce.
What decentralization risks: Loss of standardization, inconsistent documentation, and reduced audit defensibility across the organization.
The Hybrid Model: A Structured Approach to Multi-Branch RCM
Most multi-branch agencies that achieve stable reimbursement performance adopt a hybrid structure, centralizing functions where standardization drives accuracy, and retaining local control where contextual knowledge drives performance.
Functions That Must Be Centralized
- Medical coding and OASIS review: Coding accuracy under PDGM requires specialized expertise and consistent interpretation standards. Without centralized governance, interpretation drift across branch teams directly increases denial rates and complicates audit responses.
- Medicare fee-for-service billing: CMS billing requirements are uniform across locations. Centralizing Medicare billing enables standardized pre-bill validation, consistent claims submission timelines, and aggregate denial trend analysis that branch-level billing cannot produce.
- Compliance monitoring and audit readiness: A centralized compliance function must maintain consistent documentation standards, conduct uniform pre-bill audits, and respond to post-payment review requests with a coherent organizational record.
- Reporting and analytics: Denial rate analysis, AR aging, revenue forecasting, and coding accuracy metrics require consistent underlying data to be actionable. Centralized analytics produces benchmarks that are comparable across locations and over time.
Functions That Require Payer-Specific Expertise
- Managed care and commercial insurance billing: Regional plan requirements, authorization processes, and dispute resolution procedures vary enough to require payer-specific expertise. Whether that expertise sits in a branch-level team or an external partner trained on the agency's payer contracts and regional plan requirements, the requirement is knowledge, not location.
- Prior authorization management: Authorization requirements are payer-specific and frequently updated. Effective management requires staff, internal or external, with active working knowledge of each payer's current protocols and the agency's established workflows.
- Patient communication and eligibility verification: These functions require familiarity with the agency's payer mix, patient population, and care coordination processes. That familiarity can be built into an external team through documented onboarding and process training, without requiring physical proximity to the clinical team.
The hybrid model represents a structural approach that reduces denial variability while preserving operational responsiveness at the branch level.
What the hybrid model achieves: Standardization where required, flexibility where necessary, aligned to how each function actually performs.
Decision Framework: Questions Multi-Branch Agencies Must Ask
The appropriate RCM structure depends on the agency's specific operational profile. The following questions help RCM directors assess where centralization is warranted and where local control is necessary. These factors must be evaluated together rather than in isolation when determining the appropriate RCM structure.
Branch Count and Geographic Distribution
Agencies operating across three or more locations in different states or CMS jurisdictions are managing materially different regulatory environments. The greater the geographic spread, the more valuable centralized coding governance becomes, and the more important it is to retain local knowledge for payer-specific billing functions. Agencies below this threshold may find that structured branch-level processes are sufficient; those above it must treat centralized coding governance as a compliance requirement, not an operational preference.
Payer Mix Variation by Location
If each branch carries a significantly different payer mix, particularly if managed care penetration varies substantially across locations, full centralization of billing operations will create friction. Where managed care represents a significant share of a branch’s volume, typically in the 30–40% range, or where payer-specific authorization requirements drive day-to-day billing decisions, local billing expertise is operationally necessary. That threshold varies by market, but the indicator is consistent: when billing errors correlate with payer relationship gaps rather than coding gaps, centralization creates more friction than it resolves.
Technology Infrastructure
Centralized RCM requires integrated systems. If branch locations operate on different Electronic Health Record (EHR) platforms or billing systems, centralization will generate reconciliation problems rather than solve them. Technology alignment represents a prerequisite, not a byproduct. Agencies with fragmented systems must assess integration feasibility before committing to a centralized structure.
Staff Expertise and Turnover Rates
Agencies with high coding staff turnover at the branch level, a persistent challenge in home health will find centralized coding governance significantly easier to maintain than distributed competency. Turnover in a centralized team affects one function. Turnover in a decentralized model affects both operations and institutional knowledge across multiple locations simultaneously. High branch-level turnover represents a strong structural signal to centralize coding.
Agencies that map these variables before restructuring are more likely to implement sustainable RCM models that scale with growth.
Technology Requirements for Centralized RCM Operations
Centralized RCM does not function without an integrated technology infrastructure. Agencies that attempt to centralize billing and coding operations while branch locations continue to operate on disconnected systems will generate the same reconciliation gaps they were trying to eliminate.
The core requirements are consistent across organizations. Clinical documentation, OASIS data, and coding workflows must be accessible through a unified platform that maintains version control and provides a complete audit trail. Pre-bill review checkpoints verifying visit counts, service dates, required assessments, and certification completeness must be embedded in the workflow rather than managed as separate manual steps.
Reporting infrastructure must aggregate data across locations in a format that produces actionable analytics. Denial rates by branch, by payer, and by reason code must be visible at the organizational level, not reconstructed manually from branch-level reports. Claims submission timelines, AR aging by location, and coding accuracy rates must be monitored as operational metrics, not periodic audit outputs.
Agencies that integrate documentation, coding, and billing into a single platform reduce the manual handoffs where errors most commonly occur and create the data consistency that makes centralized compliance monitoring viable.
What integrated systems enable: Consistent documentation access, standardized pre-bill validation, and reliable analytics across all locations.
Change Management: Transitioning from Decentralized to Centralized RCM
Structural RCM changes in multi-branch organizations fail not because the model is wrong, but because the transition is not managed as an operational change program.
Standardize Documentation Before Centralizing Coding
The transition from decentralized to centralized RCM requires a defined sequence. Agencies must begin by standardizing documentation requirements across all branch locations before centralizing coding review. Coders working from inconsistent clinical records will produce inconsistent results regardless of governance structure.
Establish a Formal Query Infrastructure for Centralized Coding
Centralized coding teams require a formal query workflow with defined response timelines, centralized tracking, and retention as part of the compliance record. Without this, the proximity advantage that local coding teams previously provided is lost without an adequate operational replacement.
Define Decision Authority Before Running Dual Processes
Parallel operation—running centralized and branch-level processes simultaneously during transition—reduces submission risk but requires clear escalation paths. Agencies must define which team has authority over final claim decisions during the transition period and document that decision-making structure for audit purposes.
Document Accountability at Every Workflow Handoff
Staff communication represents a practical compliance consideration, not simply a change management best practice. Branch-level billing staff who are uncertain about their role after centralization will create workarounds. Documenting the new workflow, clarifying accountability at each handoff point, and establishing feedback channels between central and local teams are operational requirements, not optional enhancements.
Successful transitions require: Standardized documentation, defined workflows, and clear accountability across centralized and local teams, established before the structural change, not after.
Outsourced RCM as a Centralization Accelerator
For multi-branch agencies that lack the internal infrastructure to build a centralized RCM function, outsourcing provides a structural shortcut—not as a substitute for operational discipline, but as a means of accessing centralized expertise, technology, and compliance governance without building it from scratch.
In multi-branch environments, external RCM support is often used to standardize coding, compliance monitoring, and analytics where internal teams lack the scale to maintain consistency across locations. An outsourced RCM partner that operates at scale brings standardized coding governance, pre-built analytics infrastructure, and compliance monitoring capabilities that would take most agencies significant time and capital to develop internally.
The model works most effectively when the outsourced partner assumes responsibility not only for coding, Medicare billing, compliance monitoring, and analytics, but also for managed care billing, prior authorization, and patient communication, provided the partner's teams are trained on the agency's specific payer mix, state and regional plan requirements, and office-level workflows. The distinction that matters is not whether these functions are managed internally or externally. It is whether the team managing them, wherever they operate, has the documented payer knowledge and process familiarity to handle them accurately.
Agencies considering this approach must evaluate partners on their ability to provide dedicated teams familiar with home health and hospice coding requirements, transparent analytics reporting at the branch and organizational level, and demonstrated knowledge of CMS guidance, OASIS documentation standards, and Medicare Administrative Contractor (MAC) expectations.
In practice, multi-branch agencies typically engage external RCM support when denial variation persists across locations, internal coding governance becomes difficult to maintain, or analytics visibility is insufficient to identify root causes of revenue leakage.
Operational Example: A 12-Branch Agency Centralizes Coding, Retains Local Billing
The following scenario illustrates how a mid-sized multi-branch home health agency might structure a hybrid revenue cycle management (RCM) transition to improve operational efficiency and streamline processes. While this reflects a composite of common operational patterns rather than a named organization, the structural decisions and outcomes described are consistent with how agencies in this segment typically approach centralization.
A home health agency operating 12 branches across four states was experiencing denial rates that varied significantly between locations, from under 5% at its highest-performing branches to over 14% at its most problematic. Coding accuracy audits revealed that the variation correlated directly with branch-level coding staff turnover and the absence of a centralized interpretation standard.
The agency centralized OASIS review and medical coding under a single governance structure, with standardized query workflows, centralized tracking, and a shared reference source for coding guidelines. Medicare fee-for-service billing was consolidated into a central team with pre-bill validation checkpoints embedded in the workflow to reduce denied claims and improve cash flow.
Managed care billing, prior authorization, and patient communication were managed by teams with direct working knowledge of each location's payer mix and regional plan requirements, whether those teams were branch-level staff or external partners trained on location-specific workflows.
Within two claim submission cycles, the denial rate variance across branches narrowed significantly. Aggregate denial rates declined. Pre-bill review caught coding discrepancies before submission that had previously surfaced as post-payment audit findings. Analytics reporting at the organizational level previously unavailable because branch-level data was inconsistent became a functional management tool for the first time, providing data-driven insights to support ongoing improvement.
What changed: centralizing coding governance reduced denial variability across branches, while ensuring payer-specific expertise, not branch-level headcount, drove accuracy in managed care billing and authorization management.
A Final Perspective
The structural question for multi-branch home health agencies is not whether centralized RCM produces better outcomes than decentralized. For most compliance-sensitive functions, it does. The question is which functions belong at the center, which belong in the field, and whether the agency has the infrastructure—operational, technological, and organizational—to make that allocation work.
Agencies that approach this decision systematically—mapping functions to the layer where they perform most accurately, standardizing documentation before centralizing coding, and building analytics infrastructure that makes performance visible across locations—build RCM operations that hold as the organization grows.
Agencies that centralize without that foundation trade one set of problems for another. The structural decision matters less than the discipline with which it is implemented.
For RCM Directors and Revenue Leaders managing multi-branch home health agencies, denial variability across locations, inconsistent coding interpretation, and fragmented reporting typically represent signs of structural RCM gaps, not isolated performance issues.
Red Road supports multi-location providers with centralized coding governance, OASIS review, and compliance-focused analytics designed to reduce denial variation and improve documentation defensibility across branches.
Explore how Red Road's Revenue Cycle Management model helps multi-branch agencies standardize coding, reduce denial variability, and build centralized visibility across locations.

.webp)